The anterior cruciate ligament (ACL) is crucial for the stability and functionality of the knee joint, playing a vital role in dynamic movement and athletic performance. ACL injuries are prevalent, especially among athletes, and can lead to significant setbacks such as instability, pain, and a heightened risk of osteoarthritis. Accurate and early diagnosis is paramount to determining the most effective treatment plan and preventing further complications.
In the realm of sports medicine and orthopedics, the evolution of diagnostic tools has significantly enhanced our ability to assess the integrity of the ACL accurately. These tools range from basic physical examinations to advanced imaging techniques and robotic devices like DYNEELAX® and GNRB®. Each diagnostic method offers unique benefits and limitations, influencing treatment decisions and outcomes.
This article will explore the top six diagnostic tests for evaluating the ACL: arthroscopy, X-ray, physical examination, manual arthrometers, MRI, and robotic arthrometers. By comparing these methods through recent scientific studies, we aim to provide a comprehensive guide that assists clinicians in selecting the most appropriate diagnostic tool for ACL injuries, thereby optimizing patient care and recovery trajectories.
6) Knee Arthroscopy
Arthroscopy serves as a gold standard for diagnosing anterior cruciate ligament (ACL) injuries due to its direct visualization capabilities. This minimally invasive surgical procedure allows orthopedic surgeons to inspect, diagnose, and sometimes treat joint abnormalities inside the knee.
During an arthroscopic examination, a small camera called an arthroscope is inserted into the knee joint through a tiny incision. The camera projects images onto a screen, providing a clear view of the inside of the knee, including the ACL. Surgeons use these images to assess the extent of the injury and make real-time decisions about necessary repairs.

Advantages: The primary strength of arthroscopy lies in its accuracy and comprehensiveness. Unlike imaging tests that may miss small details, arthroscopy offers a complete evaluation of the ACL, cartilage, and other structures within the knee. This method is particularly invaluable when patient symptoms do not clearly align with clinical and imaging findings, allowing for a precise diagnosis. Additionally, arthroscopy can be both diagnostic and therapeutic, permitting the surgeon to repair or treat the injury during the same procedure, which can reduce overall recovery time and improve functional outcomes.
Disadvantages: Despite its benefits, arthroscopy is not without drawbacks. It is a surgical procedure that requires anesthesia and typically a hospital setting, introducing risks associated with surgery such as infections, bleeding, or complications from anesthesia. The procedure is also more costly than non-invasive tests and requires post-operative recovery time, during which patients may experience pain and require mobility aids. Moreover, while arthroscopy provides a detailed view of the knee’s interior, it is more invasive than other diagnostics and may lead to longer patient downtime.
In the clinical context, arthroscopy is reserved for cases where less invasive diagnostic methods fail to provide clear answers, or when simultaneous diagnostic assessment and treatment are advantageous. This selective use ensures that patients receive the most appropriate level of care without undue exposure to surgical risks.
Recent studies reinforce the value of arthroscopy not only in diagnostics but also in therapeutic interventions. For instance, it allows for the debridement (removal) of damaged tissue, which can alleviate symptoms and delay degenerative changes in the joint. Advances in arthroscopic techniques continue to reduce the invasiveness and improve the recovery times associated with the procedure, highlighting ongoing progress in ACL treatment protocols.
Conclusion: Arthroscopy remains a pivotal tool in the orthopedic arsenal for its unmatched ability to provide a definitive diagnosis and facilitate immediate treatment of ACL injuries. Its use, however, should be balanced against its invasiveness and the availability of less invasive diagnostic methods that can adequately address specific clinical needs.
5) X-Ray Imaging
X-ray imaging is a fundamental diagnostic tool often employed in the initial assessment of anterior cruciate ligament (ACL) injuries. While X-rays do not visualize the ligaments themselves, they provide invaluable information about the bony structures of the knee, which can indirectly indicate ligament damage.
During an X-ray examination, electromagnetic radiation passes through the body to produce images of the bones. This test is particularly useful for ruling out associated injuries such as fractures or bone contusions that may accompany or mimic the symptoms of an ACL injury.
Advantages: The principal benefit of X-ray imaging lies in its speed and accessibility. X-rays are widely available in medical facilities and provide a quick method for assessing the knee’s structural integrity. They are also relatively inexpensive compared to more sophisticated imaging techniques like MRI. In cases of trauma, X-rays can swiftly identify fractures that may need to be addressed immediately.
Disadvantages: The main limitation of X-rays in the context of ACL diagnostics is their inability to visualize soft tissues directly. The ACL, being a ligament, does not appear on standard X-rays as it is composed of soft tissue. Therefore, while X-rays can suggest the presence of an ACL injury through indirect signs such as the anterior tibial displacement (seen in severe injuries), they cannot confirm it alone.
The use of X-ray as a diagnostic tool for ACL injuries often must be supplemented by other diagnostic methods. Magnetic resonance imaging (MRI), for example, is commonly recommended following X-ray if a ligament injury is suspected, to confirm the diagnosis and assess the extent of damage to the soft tissues.
Key Studies:
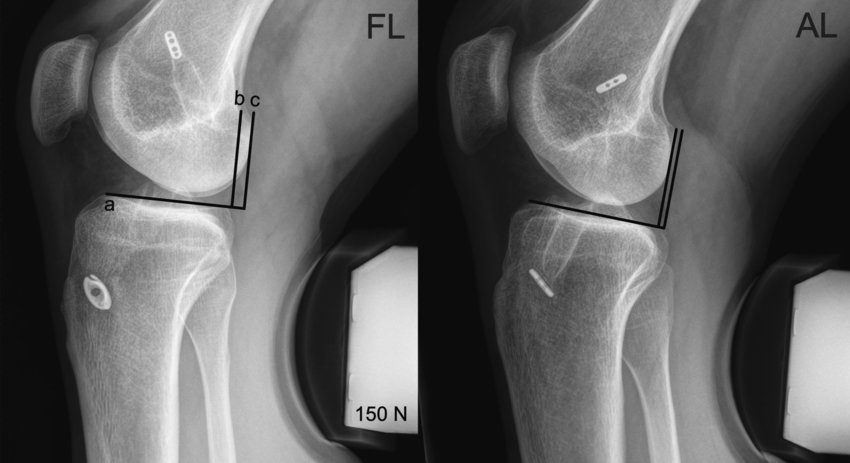
A key study highlighting the role of X-rays in ACL diagnostics is the Beldame Study (1), which meticulously compared the GNRB® arthrometer to the Telos device in stress radiography. This investigation focused on the reliability and consistency of knee laxity measurements, which are crucial for accurately assessing the integrity of the ACL.
The findings from this study were revealing; the GNRB arthrometer demonstrated a more consistent measure of knee laxity without the need for radiation exposure. This not only challenges the traditional reliance on X-ray-based Telos in regular ACL diagnostics but also highlights the potential risks associated with unnecessary radiation, especially when non-invasive alternatives can provide equal or greater accuracy.

Building on this, Lefevre Study (2) provides a compelling comparison of the GNRB® arthrometer and the Telos device in assessing partial ACL tears. Conducted over one year with 139 patients, the study demonstrated that the GNRB not only delivers more consistent anterior laxity measurements but also does so without the need for radiation, unlike the Telos.
Specifically, the GNRB® exhibited superior diagnostic accuracy, achieving an Area Under the Curve (AUC) of 0.89, indicating high reliability in diagnosing partial thickness ACL tears. These findings support a transition towards using advanced diagnostic tools like the GNRB that offer precise, safe, and non-invasive assessments, enhancing clinical decision-making in ACL injuries.
While X-ray imaging is an essential tool in the orthopedic diagnostic arsenal, its role in diagnosing ACL injuries is limited to identifying associated bony injuries and serving as a preliminary assessment method. For comprehensive ACL evaluation, X-rays must be complemented by other diagnostic techniques that can directly visualize the ligament, ensuring a thorough and accurate diagnosis.
4) Physical Examination
Physical examination remains a fundamental component of diagnosing anterior cruciate ligament (ACL) injuries. This traditional method involves a series of manual tests performed by clinicians to assess knee stability and integrity directly through physical manipulation.
During a physical examination, the most frequently used tests are the Lachman Test, the Pivot Shift Test, and the Anterior Drawer Test. Each test evaluates different aspects of knee mechanics, primarily focusing on the mobility of the tibia relative to the femur, which indicates the condition of the ACL.

Advantages: The principal strength of physical examination lies in its immediacy and simplicity. These tests require no special equipment, are cost-effective, and can be performed quickly during the initial clinical evaluation. They provide immediate feedback on the knee’s stability and are invaluable in acute settings where quick decision-making is crucial.
Disadvantages: Despite its benefits, the reliability of physical examination can be significantly influenced by the examiner’s experience and the patient’s pain response. Results can vary due to subjective interpretation and physical variability among patients, such as muscle guarding or patient discomfort, which may affect the accuracy of the tests.
Recent studies, such as the one conducted by Seung Min Ryu Study (3), highlight the inherent variability and challenges associated with manual tests. Ryu’s research meticulously compared the diagnostic accuracy of the GNRB® arthrometer with traditional physical examination methods, such as the Lachman test, which has been a longstanding benchmark for assessing ACL integrity. The study carefully analyzed both methods under controlled conditions and found that while manual tests like the Lachman are invaluable for their immediacy and simplicity, they are also prone to significant inter-examiner variability. This variability can often lead to inconsistencies in diagnosis, particularly in less clear-cut cases or when conducted by less experienced clinicians.
Ryu’s findings underscore that advanced diagnostic tools such as the GNRB® arthrometer provide more consistent and objective measurements. This device, by automating the measurement process and minimizing physical manipulation, reduces the potential for human error and the variability often seen with manual techniques. The GNRB’s ability to deliver quantitative data adds a layer of precision that physical exams alone sometimes lack. This is particularly beneficial in complex cases where the clinical presentation may be ambiguous, and where precise measurement of anterior tibial translation is crucial for an accurate diagnosis.
Furthermore, the study emphasizes the complementary nature of these tools in clinical practice. By integrating the GNRB® arthrometer’s objective data with the clinical insights gained from physical examination, clinicians can achieve a more comprehensive understanding of the knee’s condition. This integrated approach not only enhances diagnostic accuracy but also informs more tailored and effective treatment strategies, ultimately leading to better patient outcomes and a more efficient clinical workflow.
Conclusion: Physical examination is an invaluable first-line approach to diagnosing ACL injuries, yet its effectiveness can be significantly enhanced when supplemented with more objective diagnostic tools. Incorporating technology-based assessments such as the GNRB arthrometer can provide a more definitive diagnosis, supporting clinical decisions and potentially leading to better treatment outcomes.
3) Manual Arthrometers

Manual arthrometers, such as the KT1000, play a crucial role in orthopedic diagnostics by quantifying knee stability, specifically assessing the anterior cruciate ligament (ACL). These devices measure the tibial displacement relative to the femur under applied force, providing numerical indicators of knee laxity that are essential for diagnosing ACL injuries.
Description: The KT1000 arthrometer, a handheld device, allows clinicians to apply a controlled anterior force to the tibia while measuring its forward movement relative to the femur. This method is especially useful for evaluating the laxity of the ACL and is commonly used in both pre-operative assessments and post-operative follow-ups.
Advantages: The primary benefits of manual arthrometers include their ability to provide immediate, quantifiable data on knee laxity. They are straightforward to use and do not require the complex setup associated with more sophisticated diagnostic machines. Additionally, their portability makes them versatile for use in various clinical environments.
Disadvantages: The effectiveness of manual arthrometers is heavily dependent on the technique of the operator. Variability in test administration can lead to inconsistent results. These devices are also limited in their ability to detect subtle changes in laxity, particularly in cases of partial ACL tears, where accuracy is paramount. Reproducibility is also low as these devices lack sensors in parameters indicating the placement of the arthrometer on the leg.
Key Studies:
H. Robert et al. (2009) (4): This comprehensive study tested the GNRB® arthrometer’s reproducibility in comparison with the KT-1000, focusing on both complete and partial ACL tears. The study established that the GNRB® provided significantly more consistent and reproducible results across testers of varying experience levels. Specifically, at a force of 134 N, the GNRB demonstrated a sensitivity of 70% and a specificity of 99% for complete ACL tears with a differential laxity threshold of 3 mm. For partial tears, a 1.5 mm threshold improved the sensitivity to 80% and specificity to 87%. These findings suggest that the GNRB’s automated process reduces the influence of human error and variability, making it an especially reliable tool in settings where precise diagnostics are critical for effective treatment planning and monitoring rehabilitation.
Michel Collette et al. (2012) (5) : In this study, fifteen physiotherapists conducted tests on 15 subjects with healthy knees to evaluate and compare the intra- and inter-examiner reproducibility of the GNRB® against the KT-1000. Results highlighted that the GNRB® significantly outperformed the KT-1000 in terms of measurement consistency (P < 0.001), regardless of operator experience. The study emphasized the GNRB®’s technological advantages such as controlled pressure on the patella, high accuracy of displacement transducers, and automatic data recording. These features help ensure consistent application and accurate results, which are pivotal in clinical settings for ensuring reliable assessments and optimal patient outcomes
Antonio Klasan et al. (2019) (6): This investigation into the effects of laximeter type on anterior knee translation measurements post-ACL reconstruction showed that the GNRB® yielded more consistent and precise measurements than the KT1000. It was noted that the mean anterior translation of the healthy knee measured 5.7 mm with the KT1000 and 4.4 mm with the GNRB (p = 0.002), while the ACL-reconstructed knee showed 7.0 mm with the KT1000 and 5.3 mm with the GNRB (p = 0.037). The lower variance with the GNRB suggests that it provides a more reliable and stable measurement environment, potentially reducing the risk of misdiagnosis and improving the accuracy of monitoring recovery progress. The study underscores the importance of using advanced diagnostic tools in clinical settings to enhance the precision of assessments and support better clinical decision-making
Conclusion: While manual arthrometers like the KT1000 remain useful tools for assessing ACL injuries, their limitations highlight the importance of precise technique and the potential need for supplementary testing with advanced diagnostic technologies like the GNRB to ensure accuracy and reliability in ACL injury assessment.
2) Magnetic Resonance Imaging (MRI)

Magnetic Resonance Imaging (MRI) is a cornerstone in the diagnostic arsenal for anterior cruciate ligament (ACL) injuries, renowned for its high-resolution images and excellent soft tissue contrast. MRI is non-invasive and provides detailed views of both the soft and hard tissues within the knee, which makes it invaluable for assessing the extent of an ACL injury and any associated damages such as meniscal or cartilage injuries.
Description: MRI utilizes magnetic fields and radio waves to create detailed images of the body’s internal structures. For ACL assessments, it helps visualize the ligament’s integrity and the extent of the injury, which is crucial for planning treatment and surgical interventions.
Advantages: The primary benefit of MRI is its ability to provide detailed images without exposure to ionizing radiation. It offers excellent spatial resolution and the ability to evaluate multiple parameters of the knee, which is essential for a comprehensive assessment of the ACL and associated structures.
Disadvantages: Despite its benefits, MRI is not without limitations. The accuracy of MRI can vary based on the scanning technique and the experience of the musculoskeletal radiologist. Moreover, MRI scans are expensive, may have long waiting times, and the results can be influenced by the imaging angles and the specific protocol used.
Théo Cojean et al. (2023) (6): This prospective diagnostic study compared the sensitivity and specificity of MRI with the GNRB® arthrometer for detecting healthy ACL, partial, and complete ACL tears in 214 patients, with arthroscopy serving as the ‘gold standard’. The study found that while MRI showed excellent sensitivity for detecting healthy ACLs (100% sensitivity and 95% specificity), it struggled with partial ACL tears, showing only 29.51% sensitivity and 88.97% specificity. In contrast, the GNRB® demonstrated considerably higher sensitivity for partial tears at 73.77% while maintaining a comparable specificity of 85.52%. For complete ACL tears, MRI and GNRB® showed similar sensitivities (80.81% and 77.78% respectively) but the GNRB® had higher specificity (85.98% compared to 64.49% for MRI). This study highlighted that while MRI is effective for identifying complete tears and associated injuries, it may be supplemented with the GNRB® for a more accurate diagnosis of partial tears
Conclusion: MRI remains a critical tool for diagnosing ACL injuries due to its detailed imaging capabilities. However, its effectiveness can be enhanced when used in conjunction with other diagnostic tools like the DYNEELAX® and GNRB® arthrometer, especially for the challenging diagnosis of partial ACL tears. This integrated approach can provide a more comprehensive assessment, guiding more tailored and effective treatment strategies.
1) Robotic Arthrometer: GNRB & Dyneelax

Robotic arthrometers, such as the DYNEELAX® and GNRB®, offer a significant technological advancement in assessing the integrity of the anterior cruciate ligament (ACL) and overall knee laxity. These devices automate the measurement process, providing objective and reliable assessments with minimal operator dependency.
Description:
- GNRB® is designed to measure anterior tibial translation, which assesses the forward movement of the tibia relative to the femur, a key indicator of ACL integrity. This device standardizes the force application during the testing procedure, improving the consistency and accuracy of the measurements.
- DYNEELAX® not only measures anterior tibial translation but also includes capabilities for assessing tibial axial rotations, offering a more comprehensive analysis of knee mechanics. This additional functionality makes Dyneelax particularly useful in detailed diagnostic scenarios where understanding rotational laxity is crucial.
Advantages: The primary benefits of robotic arthrometers include their high precision and repeatability. They standardize the force application during testing, which is crucial for consistent measurements, and are particularly valuable in clinical settings and research for monitoring post-surgical recovery and evaluating ligament healing. Significant advantages are the following:
- ACL injury diagnosis: high precision in diagnosing the ACL through translation assessements
- Surgery Planning: Alongside translation, the rotation analysis helps determine whether extra articular plasty is necessary or not.
- Post-Op Use: these devices being controlled via a computer, it is possible to test the ACL as soon as 1 month post-op (100N) to monitor the graft and personnalize the rehabilitation.
Disadvantages: Despite their benefits, robotic arthrometers are more expensive and less portable than manual arthrometers. Their complexity also requires specific training for operators to ensure accurate usage.
Key Studies:
Magdic et al. (2023) (8): This study provides a thorough examination of the intra-rater reliability of the GNRB® knee arthrometer, affirming its consistent performance across different force applications. The researchers meticulously analyzed the device’s ability to measure knee anterior laxity, finding intraclass correlation coefficients (ICC) ranging from 0.756 to 0.848, which underscores its reliability in a clinical setting. This consistency is vital for practitioners who require dependable tools for assessing and monitoring the progression of ACL injuries and the effectiveness of rehabilitation protocols. The study also contributes to the understanding of how such measurements can influence treatment plans, providing a basis for adjusting therapeutic interventions to achieve optimal recovery outcomes. By demonstrating such high reliability, this study supports the GNRB® arthrometer’s integration into standard clinical practice for ongoing patient evaluations

Nascimento et al. (2024) (9): The research conducted by Nascimento and colleagues extensively evaluated the reliability and practicality of the Dyneelax robotic arthrometer across a cohort that included healthy individuals as well as those with ACL injuries and post-reconstruction conditions. The study highlighted the device’s exceptional reliability with ICC values between 0.91 and 0.96 across all metrics, emphasizing its robustness in clinical diagnostics. It further explored the device’s utility in providing precise and repeatable measurements of both translational and rotational knee laxity, which are critical for accurate diagnosis and assessment of knee function. This is particularly significant in settings where a comprehensive understanding of knee mechanics is crucial for developing targeted therapeutic strategies. The study also noted that the standardization of testing conditions, such as consistent knee tightening forces, significantly enhances the accuracy and reliability of measurements, advocating for standardized protocols to ensure quality control in clinical assessments
Kayla Smith et al. (2022) (10): This investigation into the GNRB® arthrometer’s performance in measuring ACL stiffness and laxity provided crucial insights into the clinical and research applications of the device. With ICC values from 0.72 to 0.83, the study affirmed the GNRB®’s capability to deliver reliable and precise measurements under controlled conditions, highlighting its potential utility in clinical trials and routine patient care. The research also delved into the implications of these measurements for designing personalized ACL rehabilitation programs, illustrating how reliable data from the GNRB® can guide clinicians in tailoring interventions to individual patient needs. Furthermore, the study presented sample size calculations, providing valuable guidelines for future research design and ensuring that studies are appropriately powered to detect meaningful differences in clinical trials
Théo Cojean et al. (2023) (11): This study rigorously evaluated the Dyneelax arthrometer’s sensitivity, repeatability, and reproducibility, providing a comprehensive assessment of its capabilities in diagnosing both partial and complete ACL injuries. By demonstrating high sensitivity in detecting subtle changes in knee laxity, the findings support the Dyneelax’s advanced diagnostic potential, particularly in challenging cases where precise measurements are crucial for accurate diagnosis and treatment planning. The study also emphasized the device’s ability to measure rotational as well as translational laxity, offering a more holistic view of knee function than many other devices. This broader diagnostic capability makes the Dyneelax particularly valuable in research settings where detailed analysis of knee mechanics is required, as well as in clinical practices focusing on complex knee injury cases
Conclusion: Robotic arthrometers like DYNEELAX® and GNRB® are crucial tools in modern orthopedic diagnostics. They offer high precision and reliability in ACL assessments, supporting their increasing use in both clinical practice and research. By integrating these advanced technologies, medical professionals can enhance diagnostic accuracy, optimize treatment plans, and improve patient outcomes.
Conclusion
The evaluation of anterior cruciate ligament (ACL) injuries has significantly evolved with technological advancements in diagnostic tools, enhancing the precision and reliability of assessments. Each of the diagnostic methods discussed—arthroscopy, X-ray, physical examination, manual arthrometers, MRI, and robotic arthrometers—plays a crucial role in the multifaceted approach required for accurate ACL injury diagnosis and management.
Arthroscopy remains the gold standard for direct visualization of the ACL, offering unparalleled detail that is crucial for definitive diagnosis and immediate therapeutic interventions. However, its invasive nature and higher costs necessitate careful consideration of its use.
X-ray and physical examinations provide valuable initial assessments but are limited by their inability to directly visualize or quantify the soft tissue structures like the ACL. Innovations such as the GNRB and newer technologies like the Dyneelax are setting new standards by offering more precise measurements and reducing the subjectivity and variability associated with traditional methods.
MRI stands out for its detailed imaging capabilities, offering excellent soft tissue contrast without radiation exposure. However, challenges in detecting partial tears and the high cost of MRI scans highlight the need for supplementary diagnostic tools.
Robotic arthrometers, particularly the DYNEELAX® and GNRB®, represent a significant advancement in the field. These devices automate laxity measurements, providing highly reliable and reproducible data that are essential for diagnosing ACL conditions accurately and monitoring treatment efficacy. The studies reviewed confirm the robustness of these tools in clinical settings, advocating for their broader adoption to enhance diagnostic accuracy and patient outcomes.
It’s important to note that robotic arthrometers are not intended to replace MRI but to complement it. Pairing both analyses—MRI for detailed imaging and robotic arthrometers for precise mechanical evaluations—offers a comprehensive approach to patient management. The ability of robotic arthrometers to measure both translation and rotation is particularly valuable; translation helps analyze the ACL directly, while rotation measurements can guide surgeons in deciding whether extra-articular plasty or a lateral extra-articular tenodesis (LET) technique is necessary. Furthermore, the ongoing monitoring of the ACL during rehabilition is only possible with robotic arthrometers, thanks to their high reproducibility and robotics.
As ACL diagnosis continues to advance, the ongoing development and validation of diagnostic technologies will be essential. Future research should focus on refining these tools, improving accessibility and cost-effectiveness, and exploring their applications in other knee-related injuries. By embracing these technological advancements, the medical community can continue to improve the standards of care provided to patients with ACL injuries.
Medical References
- Beldame, J., Mouchel, S., Bertiaux, S., & Adam, J.M. (2012). Anterior knee laxity measurement: Comparison of passive stress radiographs Telos® and ‘‘Lerat’’, and GNRB® arthrometer. Orthopaedics & Traumatology: Surgery & Research, 98, 744-750. DOI: 10.1016/j.otsr.2012.05.017
- Lefevre, N., Bohu, Y., Naouri, J.F., Klouche, S., & Herman, S. (2013). Validity of GNRB arthrometer compared to Telos in the assessment of partial anterior cruciate ligament tears. Knee Surgery, Sports Traumatology, Arthroscopy, 22, 285-290. DOI: 10.1007/s00167-013-2384-4
- Ryu, S.M., Park, J.W., Na, J.B., Lim, H.T., & Bae, J.H. (2018). Diagnostic Tools for Acute Anterior Cruciate Ligament Injury: A Comparative Study. The Knee, 25, 414-420. DOI: 10.5792/ksrr.17.014
- Robert, H., Nouveau, S., Gageot, S., & Gagnière, B. (2009). A new knee arthrometer, the GNRB: Experience in ACL complete and partial tears. Orthopaedics & Traumatology: Surgery & Research, 95, 171-176. DOI: 10.1016/j.otsr.2009.03.009
- Collette, M., Courville, J., Forton, M., & Gagnière, B. (2012). Objective evaluation of anterior knee laxity; comparison of the KT-1000 and GNRB arthrometers. Knee Surg Sports Traumatol Arthrosc. DOI: 10.1007/s00167-011-1869-2.
- Klasan, A., Putnis, S.E., Kandhari, V., Oshima, T., & Parker, D.A. (2019). Anterior knee translation measurements after ACL reconstruction are influenced by the type of laximeter used. Knee Surgery Sports Traumatology Arthroscopy. DOI: 10.1007/s00167-020-05950-5.
- Cojean, T., Batailler, C., Robert, H., & Cheze, L. (2023). GNRB® laximeter with magnetic resonance imaging in clinical practice for complete and partial anterior cruciate ligament tears detection: A prospective diagnostic study with arthroscopic validation on 214 patients. The Knee. DOI: 10.1016/j.knee.2023.03.017.
- Magdić M, Gošnak Dahmane R, Vauhnik R. (2023). Intra-rater reliability of the knee arthrometer GNRB® for measuring knee anterior laxity in healthy active subjects. Journal of Orthopaedics. DOI: 10.1016/j.jor.2023.03.016
- Nascimento, N., Kotsifaki, R., Papakostas, E., Zikria, B. A., Alkhelaif, K., Hagert, E., Olory, B., D’Hooghe, P., & Whiteley, R. (2024). DYNEELAX Robotic Arthrometer reliability and feasibility on healthy and anterior cruciate ligament injured/reconstructed persons. Translational Sports Medicine, 2024, Article ID 3413466, 1-5. DOI: 10.1155/2024/3413466
- Smith K, Miller N, Laslovich S. (2022). The Reliability of the GNRB® Knee Arthrometer in Measuring ACL Stiffness and Laxity: Implications for Clinical Use and Clinical Trial Design. Int J Sports Phys Ther, 17(6), 1016-1025. DOI: 10.26603/001c.38252
- Cojean, T., Batailler, C., Robert, H., Cheze, L. (2023). Sensitivity repeatability and reproducibility study with a leg prototype of a recently developed knee arthrometer: The DYNEELAX®. Medicine in Novel Technology and Devices, 19, 100254. DOI: 10.1016/j.medntd.2023.100254